Is TLIF a major surgery?
TLIF surgery should be considered a major surgery as it involves general anesthesia and placement of a cage, screws, and rods. Minimally invasive TLIF, however, decreases the surgical invasiveness and enhances recovery rates.
What is a minimally invasive TLIF?
Minimally invasive TLIF utilizes much smaller incisions compared to traditional open surgery and has been shown to cause less muscle dissection, reduced postoperative pain, and faster recovery and return to activities. It also sometimes takes advantage of expandable cage technology.
How is TLIF surgery performed?
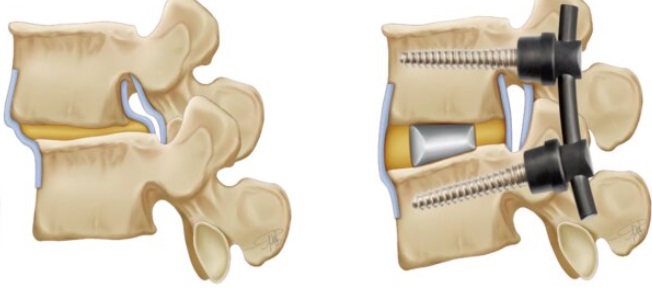
The patient is placed prone (lying flat, face downwards) under general anesthesia and an incision is made at the affected spinal level. Spinal facets are removed on one side which gives access to the disc space. A part of the intervertebral disc is then removed, and then the cage, screws and rods are placed.
What is a TLIF cage?
A TLIF cage works as a spacer after a portion of the disc between the vertebrae is removed as part of the procedure. It is made of carbon fiber, polyetheretherketone (PEEK), or trabecular metal and is filled with bone graft to enhance fusion of the vertebrae.
What is the recovery time for TLIF surgery?
The typical recovery time for TLIF surgery ranges from 6 to 12 weeks, although it varies from patient to patient. Most people are off pain medications and can return to work and driving within two weeks.
How soon can you walk after a TLIF surgery?
Patients typically start walking the same day after TLIF surgery.
Do you need physical therapy after a TLIF surgery?
Physical therapy (PT) is generally beneficial after TLIF surgery. It reduces the pain and inflammation, strengthens the back, and assists the patient in a graded recovery after surgery.
What risks or complications can occur with TLIF surgery?
Possible problems can include bleeding, infection, injury to the nerves, or a need for a reoperation (revision surgery). Bleeding and infection are rare (less than 1%) in a minimally invasive TLIF. Reoperations (additional revision surgeries) may be needed in about 10% to 15% of cases in the event of complications like failure of fusion or adjacent segment degeneration. (Because fusion eliminates motion at a particular spinal segment, adjacent segments compensate for lost motion by increasing their mobility. This puts them under added stress and can make them prone to accelerated degeneration, as compared to the natural rate of degeneration as people age.)